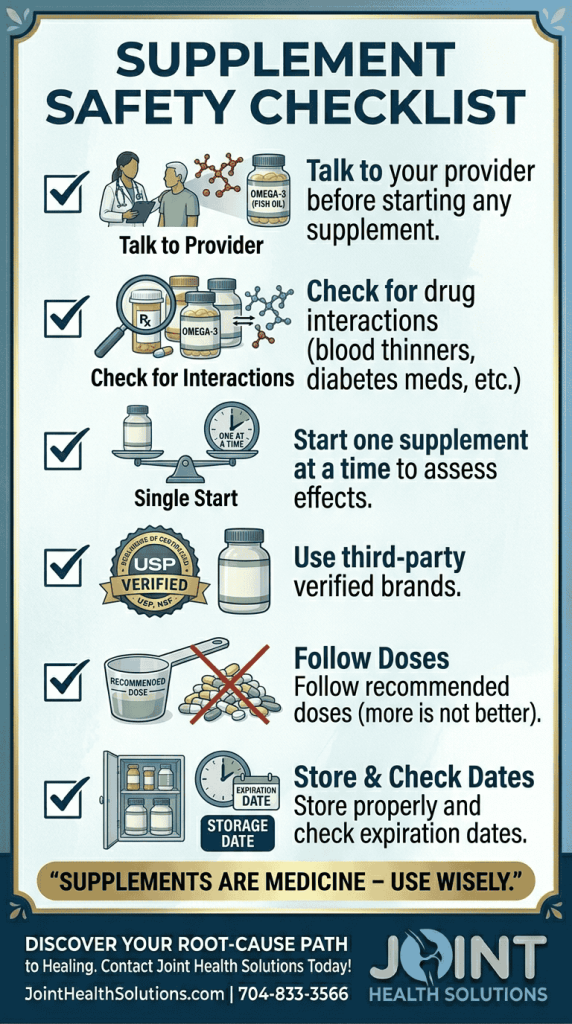
This article is for educational purposes only. It is not medical advice, and it does not constitute a recommendation or prescription from Joint Health Solutions. We do not sell, prescribe, or recommend specific supplements. We do not perform supplement-related testing (such as vitamin D levels or omega 3 index). If you are considering taking any supplement, please consult your primary care provider or a registered dietitian. Some supplements can interact with medications (blood thinners, diabetes drugs, chemotherapy) or cause side effects.
Important note: Supplements are not a replacement for medical treatment. They work best as part of a comprehensive plan that includes diet, exercise, and – when needed – advanced therapies like PRP Therapy or hyaluronic acid injections.
Many individuals with osteoarthritis, tendinopathy, or other joint conditions turn to supplements for several reasons:
However, supplements are not a substitute for medical treatment. They work best alongside, not instead of, evidence based therapies such as PRP, hyaluronic acid injections, physical therapy, bracing, and IV therapy. This guide summarizes the current scientific evidence so you can have an informed discussion with your doctor.
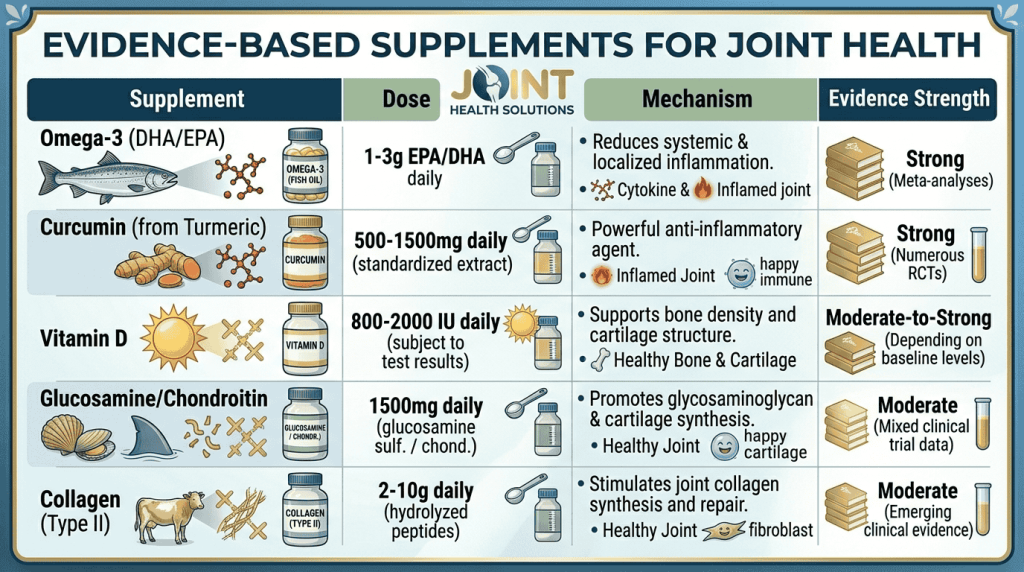
The following supplements have been studied in clinical trials. The evidence varies in quality. Discuss these options with your healthcare provider.
What they do: Omega 3s reduce the production of inflammatory prostaglandins and cytokines. They are well known for their cardiovascular benefits, but they also have anti inflammatory effects that may help with joint pain.
What research shows: Clinical and pre clinical studies indicate that omega 3 polyunsaturated fatty acids (PUFAs) reduce inflammatory markers and may protect against cartilage loss in osteoarthritis. A narrative review published in Nutrients concluded that omega 3s have anti inflammatory effects and potential to moderate pro inflammatory markers and cartilage loss.
Typical dose used in studies: 1–3 grams of EPA/DHA daily.
Sources: Fatty fish (salmon, sardines, mackerel), fish oil supplements, or algae oil (vegan).
Safety considerations: Possible fishy aftertaste, mild gastrointestinal upset. High doses (>3g daily) may increase bleeding risk. If you take blood thinners (warfarin, apixaban, etc.), consult your doctor before starting.
What it does: Curcumin is the active compound in turmeric. It blocks NF κB and COX 2 pathways, similar to ibuprofen, but with fewer gastrointestinal side effects.
What research shows: A double blind randomized multicenter trial found that Curcuma domestica extracts were as effective as ibuprofen for knee osteoarthritis, with significantly fewer stomach complaints. However, curcumin is poorly absorbed on its own. Look for products with piperine (black pepper extract) or liposomal formulations.
Typical dose used in studies: 500–1000 mg of standardized curcumin (95% curcuminoids) daily, taken with piperine.
Sources: Supplements (curcumin extract), not dietary turmeric (which contains very low amounts of curcumin).
Safety considerations: Mild GI upset; may interact with blood thinners. Avoid if you have gallbladder disease unless approved by your doctor.
What it does: Vitamin D modulates immune function, reduces inflammation, and supports bone and cartilage health. Deficiency is extremely common in people with arthritis.
What research shows: A systematic review reported that vitamin D administration improves quality of life, reduces pain perception, enhances muscle strength, and lowers inflammation in patients with knee osteoarthritis. The optimal blood level is generally considered 50–80 ng/mL.
Typical dose used in studies: 2000–5000 IU daily, but dosing should be based on blood testing. Do not take high doses without knowing your level.
Sources: Sunlight, fatty fish, supplements (vitamin D3 is more effective than D2).
Safety considerations: Rare at moderate doses; toxicity possible with excessive intake (>10,000 IU/day long term). Always test before starting high doses.
What they do: These are natural components of cartilage. The theory is that supplementing them may provide building blocks for cartilage repair and have mild anti inflammatory effects.
What research shows: Evidence is mixed. The large GAIT trial (2006) found no significant benefit overall, but a subgroup with moderate to severe knee pain did improve. A later trial (MOVES, 2016) reported that the combination was as effective as celecoxib (Celebrex) for knee osteoarthritis pain and swelling. Overall, any benefit appears modest.
Typical dose used in studies: Glucosamine 1500 mg/day + chondroitin 800–1200 mg/day.
Sources: Shellfish (glucosamine) or vegetarian (fermented corn). Avoid shellfish derived glucosamine if you have a shellfish allergy.
Safety considerations: Mild GI upset. Some studies suggest glucosamine may affect blood sugar; monitor if diabetic.
What it does: Provides amino acids (glycine, proline, hydroxyproline) that may stimulate cartilage and bone repair.
What research shows: A systematic review of randomized controlled trials reported beneficial outcomes of hydrolyzed collagen supplementation, including pain reduction, improvements in clinical parameters, and increased physical mobility in people with osteoarthritis. However, effective doses are high – at least 10 grams daily.
Typical dose used in studies: 10–20 grams of hydrolyzed collagen peptides daily.
Sources: Bovine (cow), marine (fish), or chicken collagen.
Safety considerations: Rare; mild GI upset. Low dose products (2–5 g) are unlikely to help.
The following supplements have some positive studies, but evidence is not as strong. They may help some individuals, but they should not be first line options.
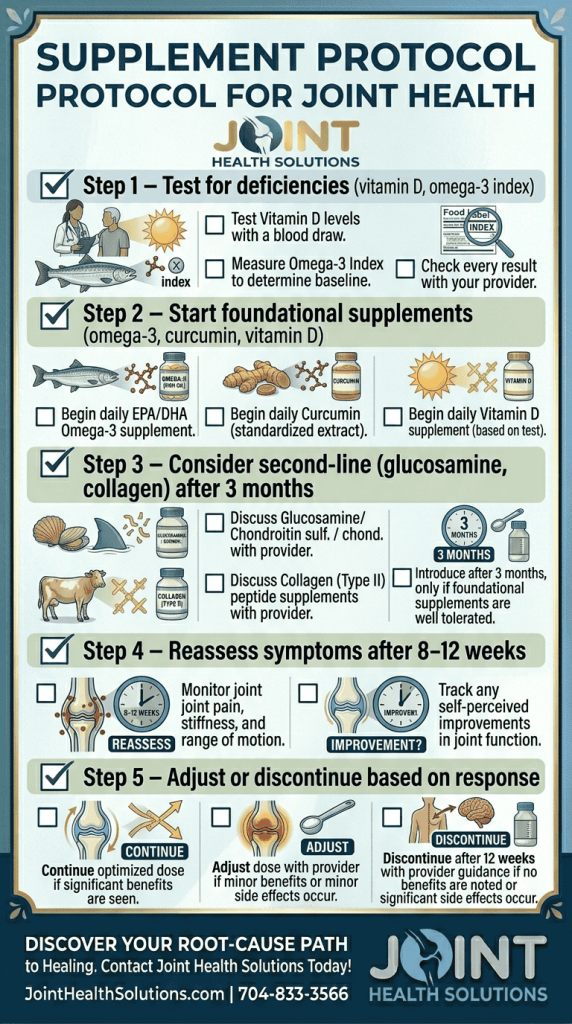
Our approach: We may recommend these as second‑line options if first‑line supplements (omega‑3, curcumin, vitamin D) are insufficient or not tolerated.
The supplement industry is poorly regulated. Follow these tips:
When in doubt, ask us – we can recommend specific brands and formulations.
We focus on treatments with stronger evidence for structural joint problems: PRP therapy, hyaluronic acid injections, fluoroscopy guided cortisone injections, offloading knee braces, and anti inflammatory IV therapy. These treatments address the joint directly. Supplements, if used at all, should be considered supportive – not primary – and you should discuss them with your primary care provider.
At Joint Health Solutions, we integrate supplement recommendations into your personalized plan – never as a standalone “magic bullet.”
No, we do not sell any supplements. This guide is purely educational.
No. Supplements may help mild symptoms but cannot reverse structural damage like cartilage loss or repair torn tendons.
Some studies suggest it may affect blood sugar. Monitor closely if you try it, and consult your endocrinologist.
Typically 2 3 months. If you experience no improvement in pain, stiffness, or function after 3 months, it is unlikely to help.
Yes, but introduce them one at a time (2 4 weeks apart) to assess tolerance and effectiveness.
Not necessarily. Look for third party certification rather than price. A moderately priced certified product is better than an expensive uncertified one.
Most people cannot. You would need 2 3 servings of fatty fish (salmon, sardines, mackerel) per week. Supplementation ensures consistent dosing.
ALA converts poorly to EPA/DHA (under 10%). Algae based DHA/EPA is a better vegan option.
It is safer to test first. Ask your primary care provider for a 25 hydroxy vitamin D blood test.
No, we do not endorse any brand. Follow the quality tips in this article.
Omega 3, curcumin, and high dose vitamin E may increase bleeding risk. Always tell your doctor and pharmacist about all supplements you take.
See the sources below from Harvard, Johns Hopkins, Mayo Clinic, and NIH. Also search PubMed for primary studies.
Yes, vegetarian glucosamine (fermented corn) is available. Avoid shellfish derived versions.
Keep a symptom diary. Stop the supplement and consult your doctor if you experience nausea, diarrhea, rash, or unusual bleeding.