Degenerative Joint Disease (DJD), also known as osteoarthritis (OA), is the most common form of arthritis, affecting about 33 million U.S. adults. It develops when the cartilage that cushions the ends of bones begins to break down, causing pain, stiffness and swelling.
Although OA was once thought of as inevitable “wear and tear,” researchers now recognize that chronic low‑grade inflammation, metabolic factors, biomechanical stresses and even gut dysbiosis contribute to its development and progression. At Joint Health Solutions, we take a proactive, root‑cause approach to DJD—focusing on prevention, early intervention and minimally invasive treatments to help you stay active and avoid joint replacement.
Osteoarthritis is a chronic joint disease characterized by the breakdown of articular cartilage. As cartilage deteriorates:
OA most commonly affects the knees, hips, hands, spine and shoulders, but any synovial joint can be involved.
Radiologists use the Kellgren–Lawrence (KL) grading system to classify the severity of osteoarthritis on X‑rays. Early detection (Grades 1‑2) offers the best opportunity for disease‑modifying interventions.
Grade | Description | X‑Ray Findings | Typical Symptoms |
0 | No osteoarthritis | Normal joint space | None |
1 | Doubtful narrowing | Possible joint space narrowing; possible small bone spurs | Occasional mild pain |
2 | Mild OA | Definite bone spurs; possible reduced joint space | Pain with activity; morning stiffness |
3 | Moderate OA | Definite moderate joint space narrowing; multiple bone spurs; possible deformity | Frequent pain, crepitus, stiffness |
4 | Severe OA | Severe joint space narrowing; large bone spurs; deformity | Constant pain; limited range of motion |
Source: Kellgren–Lawrence grading descriptions.
Several factors increase your risk of developing osteoarthritis. These factors interact; addressing modifiable risks can slow disease progression.
Risk Factor | Mechanism |
Age | Cartilage becomes less resilient with age; cumulative mechanical wear increases risk. |
Obesity | Excess body weight loads joints (each pound of weight adds four pounds of force on knees) and fat tissue releases inflammatory cytokines that accelerate cartilage damage. |
Joint Injury | Previous trauma (e.g., ACL tears) or repetitive stress damages joint structures, accelerating OA. |
Genetics | Family history of OA increases susceptibility. |
Gender (Female) | Women are more likely to develop OA, especially after menopause, possibly due to hormonal and anatomical factors. |
Muscle Weakness | Weak quadriceps and other supporting muscles reduce joint stability and are associated with increased knee pain. |
Obesity & Gut Dysbiosis | Obesity and an imbalanced gut microbiome cause systemic inflammation and release of inflammatory proteins that settle in the joint lining. |
Low Vitamin D | Low vitamin D levels are associated with reduced knee cartilage volume and increased OA progression. |
You can’t change your age or genetics, but you can reduce your risk or slow disease progression by adopting these strategies:
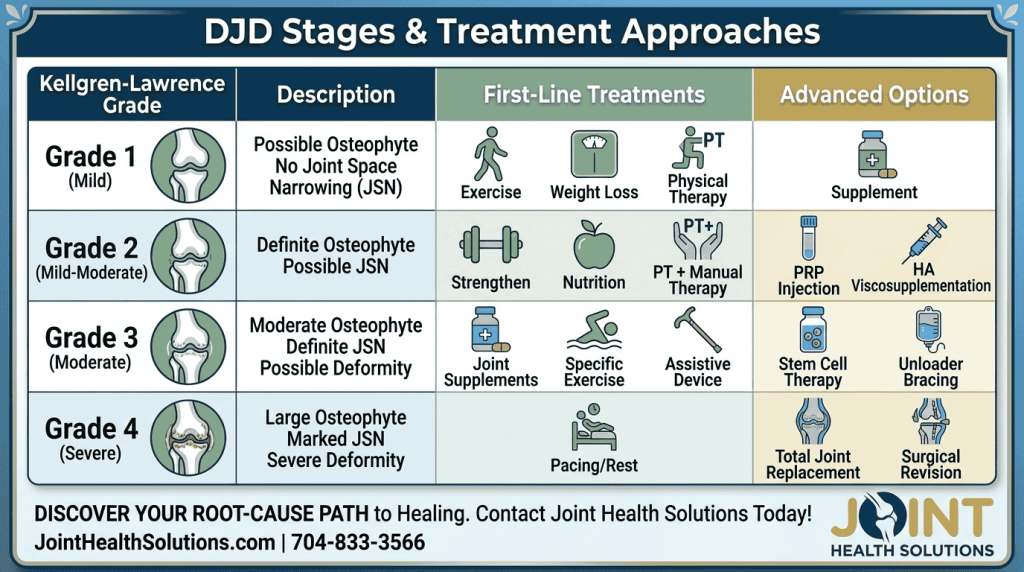
Most patients with Degenerative Joint Disease (DJD) can be managed successfully without surgery. We offer a full spectrum of non-surgical treatments to help you stay active:
Injections for Pain Relief: For acute flares, Cortisone Injections provide rapid but temporary relief. To lubricate the joint and relieve symptoms for 6–12 months, we also provide Hyaluronic Acid Injections.
Regenerative Medicine: We utilize PRP Therapy to stimulate healing, which may help slow the loss of cartilage in patients with Degenerative Joint Disease (DJD).
Supportive IV Therapies: To reduce systemic inflammation, we offer Anti-Inflammatory IV Therapy. Additionally, you can visit our page on IV NAD+ Therapy to learn how it supports cellular energy and mitochondrial health.
Bracing: In specific cases, Offloading Knee Braces can be used to redistribute weight and reduce pressure on the damaged joint compartment.
Surgery is reserved for patients with severe osteoarthritis (Grade 4) who have failed comprehensive non‑surgical management and have significant pain or functional limitations. Options include:
Degenerative joint disease is chronic but doesn’t have to define your life. These habits and monitoring strategies help maintain function and reduce pain:
If you’re ready to uncover the root cause of your joint pain and start your healing journey, schedule your first appointment today. Visit our New Patient Forms, learn more about what to expect here, or call us at 704-833-3566 to speak with our team. We’re here to help you take the first step toward relief and wellness.
Yes. The terms are used interchangeably.
No, but progression can be slowed and symptoms managed with early intervention and lifestyle changes.
No. Appropriate low‑impact exercise strengthens muscles, improves stability and reduces pain.
An anti‑inflammatory diet rich in omega‑3s (fatty fish, walnuts), antioxidants (berries, leafy greens) and phytonutrients (turmeric, ginger). Avoid excess sugar and processed foods.
Studies show PRP can reduce pain and improve function for 6–12 months, especially in mild to moderate knee OA; it may also slow cartilage loss.
Typically every 6–12 months, depending on the product and your response.
When non‑surgical options have failed and pain significantly impacts daily activities (e.g., can’t walk more than a block or sleep comfortably).
You can’t change your genes, but maintaining a healthy weight, avoiding joint injuries, staying active and controlling inflammation reduce your risk.
Evidence is mixed; some patients experience benefit while others don’t. It’s generally safe to try for 3 months.
Call our office or book online to schedule a consultation. We’ll assess your stage, identify modifiable risk factors and create a personalized plan.
Explore these authoritative sources for more in-depth information on Osteoarthritis and treatment standards:
American Academy of Orthopaedic Surgeons – Osteoarthritis of the Knee Visit OrthoInfo by AAOS
Arthritis Foundation – Osteoarthritis Treatment Guidelines View Treatment Guidelines
Mayo Clinic – Osteoarthritis: Diagnosis and Treatment Read Clinical Overview
Osteoarthritis and Cartilage Journal – Kellgren–Lawrence Grading System Study Access Research Paper (DOI)