
Knee pain stands as one of the primary reasons adults seek specialized medical care, and a degenerative meniscus tear is an exceptionally frequent culprit—particularly in individuals over the age of 40. Unlike an acute, traumatic meniscus tear that occurs abruptly during sports from a sudden twist, pivot, or direct impact, a degenerative tear develops gradually over time. As the body ages, the cellular composition of the meniscus changes: it naturally loses its structural water content, becomes progressively less flexible, and begins to fray under the strain of ordinary daily activities.
For many decades, arthroscopic knee surgery—specifically a partial meniscectomy to trim away the damaged cartilage tissue—was considered the automatic, default response to these tears. However, modern interventional orthopedics has undergone a massive paradigm shift. High-quality, multi-center randomized clinical trials have conclusively proven that for degenerative meniscus tears that do not present with acute mechanical locking, comprehensive non-surgical management produces long-term patient outcomes that are entirely equal to surgery. By opting for conservative care, patients achieve the same pain relief and functional restoration while completely bypassing the inherent risks of anesthesia, post-operative infections, surgical downtime, and accelerated joint arthritis.
At Joint Health Solutions, we focus on delivering evidence-based, non-surgical management strategies for complex knee conditions, including complex degenerative meniscus tears. This comprehensive guide details the structural science behind degenerative cartilage fraying, explores what modern clinical research reveals about arthroscopy, outlines our multi-phase non-surgical recovery pathways, and highlights exactly when a surgical consultation remains medically necessary.
To understand how a tear develops without a clear accident, it helps to review the anatomy of the knee. The meniscus is a specialized, C-shaped wedge of dense fibrocartilage that functions as the primary shock absorber between your thighbone (femur) and shinbone (tibia). Each of your knee joints contains two distinct menisci:
The Medial Meniscus: Situated on the inner side of the knee joint, this structure bears a massive portion of your everyday walking load.
The Lateral Meniscus: Positioned on the outer side of the knee, providing vital rotational stability.
As part of the natural aging process, the meniscus experiences a gradual loss of its internal water content and structural collagen integrity, which makes the fibrocartilage more brittle and less resilient. A degenerative meniscus tear occurs when this weakened cartilage tissue slowly frays, splits, or develops horizontal delamination—frequently without any history of a sports injury or distinct physical trauma. Instead, a patient might simply step out of a car, rise from a low squat while gardening, or simply walk across a level room and suddenly feel a sharp twinge, click, or pop.
To help you understand your diagnosis, the table below highlights the key differences between age-related degenerative wear and acute traumatic tears:
| Diagnostic Feature | Degenerative Meniscus Tear | Traumatic Meniscus Tear |
| Typical Age Group | Primarily observed in individuals >40 years old | Can occur at any age; most common in younger athletes |
| Underlying Mechanism | Minimal, normal, or zero physical trauma | Sports-related injuries involving sharp twisting, pivoting, or sudden deceleration |
| Symptom Onset | Gradual, creeping, and intermittent over months | Sudden, sharp, well-defined injury timeline |
| Associated Osteoarthritis |
Almost always present concurrently within the joint | Frequently absent; surrounding joint structures are healthy |
| Mechanical Locking/Catching | Rare; typically presents as an achy or clicking sensation | Much more common due to unstable, loose tissue flaps |
The clinical preference for immediate surgery was challenged by the publication of several key orthopedic trials, including the landmark METEOR (Meniscal Tear Injury Treatment) study and multiple long-term randomized controlled trials published in the New England Journal of Medicine. These comprehensive investigations followed hundreds of patients to compare arthroscopic partial meniscectomies against standardized, non-surgical physical rehabilitation protocols.
The key scientific findings from these years of research include:
Functional Equivalence: In patients presenting with a degenerative meniscus tear and mild-to-moderate knee osteoarthritis, physical therapy alone was proven to be non-inferior to surgical intervention when measured at 6, 12, and 24 months.
No Added Value from Surgery: Patients who underwent arthroscopic surgery followed by physical therapy achieved no better long-term pain relief, mobility gains, or quality-of-life scores than those who used targeted physical therapy alone.
High Success Rates for Conservative Care: Cross-over from the conservative treatment group to the surgical group occurred in only about 30% of participants. This means that 70% of patients successfully avoided knee surgery entirely by sticking with a high-quality conservative rehabilitation program.
Arthritis Progression Dynamics: While arthroscopic cleaning did not show an immediate acceleration of joint arthritis in every patient, removing sections of the meniscus reduces the joint’s surface area, which can increase long-term stress on the remaining bone. Crucially, surgery did absolutely nothing to prevent or slow down the ultimate development of joint arthritis.
The clinical conclusion across the international orthopedic community is definitive : Every evidence-based protocol should begin with comprehensive, non-surgical care. Surgical consideration should be strictly reserved for patients exhibiting severe, unmanageable mechanical blockages (such as a locked joint) or those who show zero improvement after 3 to 6 months of high-quality conservative care.
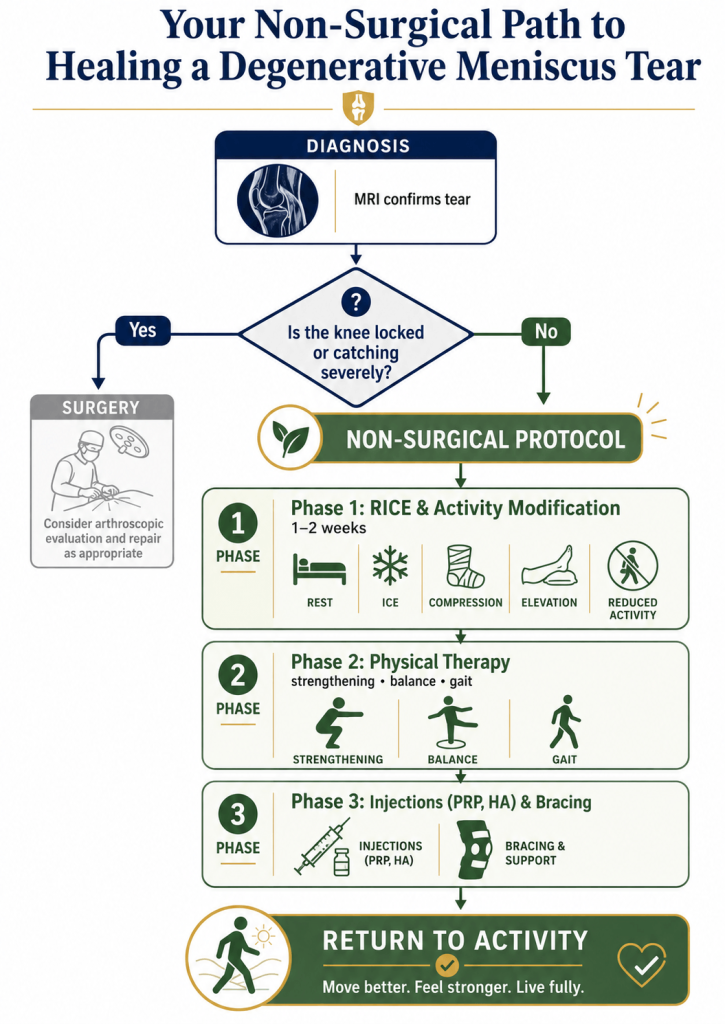
Most patients diagnosed with a degenerative meniscus tear can successfully return to their favorite activities without an operation. At Joint Health Solutions, we design a customized, multi-phase therapeutic pathway tailored to your specific anatomy and lifestyle goals:
The immediate goal during an acute pain flare-up is to calm local tissue inflammation and minimize swelling inside the joint capsule.
Rest: This does not mean complete bed rest or locking the leg straight in an immobilizer brace, which can cause muscle stiffness. Instead, avoid movements that cause sharp pain, such as deep knee bends, sudden pivoting, or heavy lifting. Walking short distances on flat, level surfaces is safe and encouraged.
Ice: Apply cold packs for 15 to 20 minutes, 3 to 4 times a day, to reduce swelling and numb local pain pathways.
Compression: Wearing a lightweight, medical-grade elastic knee sleeve can help manage swelling and improve joint spatial awareness (proprioception).
Elevation: Whenever you are resting, prop your leg up so your knee rests slightly above the level of your heart to encourage proper fluid drainage.
Supervised physical rehabilitation serves as the foundation of successful non-surgical meniscus recovery. A skilled physical therapist works to balance the mechanical forces across your leg:
Targeted Strengthening: Focused exercises build strength in your quadriceps, hamstrings, and gluteal muscles. Stronger muscle groups act as an external braking system, absorbing everyday movement impacts and reducing the direct load placed on your healing meniscus.
Proprioceptive Training: Balance exercises help stabilize your knee, preventing unexpected twisting or micro-pivoting forces that can irritate the tear.
Gait Analysis and Correction: Adjusting movement patterns helps eliminate limping or knee wobbling, protecting both legs from uneven wear.
Ergonomic Coaching: Learning safer ways to squat, lift, and climb stairs helps protect your knee cartilage during daily tasks.
Most patients complete a 6 to 12-week rehabilitation program, with a large majority noticing significant improvements in stability and pain reduction by week 8.
If localized pain or swelling limits your progress during physical therapy, we can introduce specialized, minimally invasive medical interventions to support your recovery:
📋 Advanced Non-Surgical Directives
* Precision Cortisone Injections: Designed for sudden, severe inflammation flares, a targeted injection provides rapid, temporary cooling of joint inflammation, making physical therapy much more comfortable. * Hyaluronic Acid (HA) Viscosupplementation: This option adds a lubricating fluid layer inside your joint capsule, reducing friction and soothing discomfort from concurrent osteoarthritis. Learn more about this treatment on our Hyaluronic Acid Injections page. * Platelet-Rich Plasma (PRP) Therapy: Emerging clinical data shows that autologous PRP injections can introduce valuable growth factors that support tissue healing, particularly within the outer “red zone” of the meniscus, which maintains a direct blood supply. Explore the details on our PRP Therapy platform. * Offloading Knee Bracing: A custom-calibrated unloader brace can subtly shift your weight-bearing forces away from the torn section of the meniscus, which is especially helpful for relieving inner (medial) knee pain. Review these devices on our Offloading Knee Braces page.
Once your knee meets key clinical milestones—including a complete absence of swelling, full range of motion, stable quadriceps strength (such as performing a straight leg raise without lagging), and pain-free walking on flat surfaces—you can begin a phased return to sport. You will transition from low-impact activities like road cycling or elliptical training back into more demanding movements, such as jogging or recreational sports, under the guidance of your care provider.
While conservative options are highly effective for most degenerative cases, arthroscopic surgery (such as a partial meniscectomy or meniscus repair) remains necessary in specific situations:
True Mechanical Locking: This occurs when a displaced fragment of torn meniscus cartilage physically jams inside the hinge mechanism of the joint, making it impossible to fully straighten the leg (often due to a bucket-handle tear). This is an urgent issue that requires prompt orthopedic care.
Persistent Conservative Failure: When a patient completes 3 to 6 months of structured physical therapy, custom bracing, and appropriate injections but continues to experience structural catching, regular buckling, or disabling pain that prevents daily activities.
Unstable Tears in Younger Patients: Large, unstable tears occurring in younger, active individuals who do not show signs of underlying joint osteoarthritis.
Even when surgery is required, we often recommend pre-operative physical therapy (“pre-hab”) to build muscle strength, which can help speed up your post-operative recovery.
At Joint Health Solutions, we take a balanced, measured approach rather than rushing into surgery. Our comprehensive care model focuses on:
The inner two-thirds of the meniscus structure (known as the “white zone”) lacks a direct blood supply, meaning it does not regenerate or “knit back together” on its own. However, a lack of structural healing does not mean you will always have pain. As local inflammation subsides and the surrounding leg muscles are strengthened through targeted exercise, most patients become completely symptom-free and regain full function.
For mild-to-moderate degenerative fraying, most patients achieve meaningful pain relief and return to normal activity within 4 to 8 weeks of starting a targeted physical therapy program. For more chronic, long-standing tears accompanied by joint arthritis, a full recovery can take 3 to 6 months of consistent, multi-modal care.
Typically, no. Crutches are rarely necessary for degenerative meniscus tears because most patients can bear weight safely. They are generally reserved for brief periods of severe, acute pain flares or when a mechanical tear causes the joint to lock.
We advise pausing high-impact running routines during the early stages of your recovery until you can demonstrate a full, pain-free range of motion, zero swelling, and balanced quadriceps strength. Many runners are able to safely return to their sport by combining physical therapy with a supportive offloading knee brace.
Clinical evidence for Platelet-Rich Plasma therapy is encouraging, though research is ongoing. PRP tends to be most effective when applied to tears located in the vascular outer “red zone” of the meniscus or when used to manage pain in knees with concurrent mild-to-moderate osteoarthritis.
During the initial recovery phase, you should avoid deep squats, lunges where the knee bends beyond 90 degrees, repetitive heavy lifting, and sports that require rapid pivoting or twisting (such as basketball, soccer, or singles tennis). Your physical therapist will help you identify safe, lower-impact modifications.
Yes, a high-quality offloading brace can be very helpful. By shifting weight-bearing loads away from the injured section of cartilage, it reduces mechanical stress on the tear, helping you stay active and exercise comfortably during physical therapy.
If you have completed 3 to 6 months of dedicated physical therapy, combined with appropriate injections or bracing, but still experience disabling pain, regular catching, or structural locking that interferes with daily life, a surgical consultation may be appropriate.
Degenerative tears usually occur in joints that already show early signs of age-related osteoarthritis. Opting for surgical removal of meniscus tissue (a meniscectomy) can actually accelerate arthritis progression by reducing the joint’s natural shock absorbers, which is why a non-surgical approach is recommended first.
Getting started is simple. Contact our office or use our online scheduling portal to arrange an initial consultation. Our specialist team will thoroughly evaluate your knee, review your MRI images, and design a personalized conservative care plan tailored to your lifestyle.

A board-certified physician in Emergency Medicine and Obesity Medicine with over 25 years of experience

A board-certified Family Nurse Practitioner with over 12 years of nursing experience
