What to Expect During Your First Visit to a Functional Medicine Joint Clinic
If you’ve been living with chronic joint pain and feel like conventional medicine has only offered band‑aids—painkillers, cortisone shots, or the prospect of surgery—you may be ready for a different approach. Functional medicine looks beyond the joint to find the root cause of your pain, whether it’s hidden inflammation, gut dysfunction, hormonal imbalances, or nutritional deficiencies.
But what actually happens during a functional medicine joint consultation? It’s not a typical 10‑minute visit where you leave with a prescription. It’s a comprehensive, collaborative process that sets the stage for lasting healing.
At Joint Health Solutions, we’ve designed our first visit to be thorough, respectful of your time, and focused on uncovering the real drivers of your pain. Here’s what you can expect.
Before Your Appointment
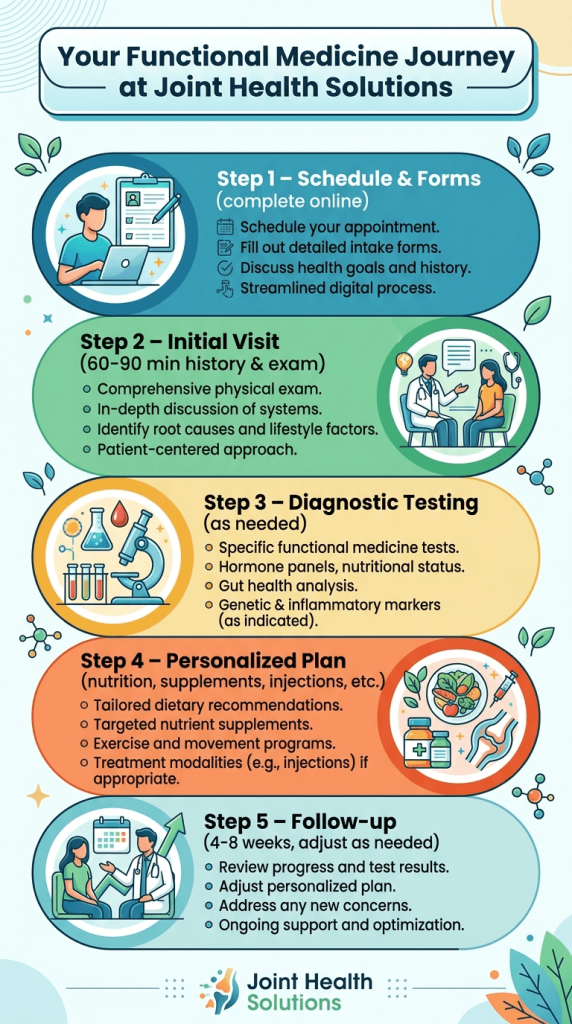
Once you schedule your first visit, we’ll send you a new patient packet that includes:
- Detailed medical history forms
- Joint pain and symptom questionnaires
- Lifestyle and diet assessment
- Authorization for release of prior medical records (if applicable)
We ask that you complete these forms online before your appointment. This allows us to review your history in advance and make the most of our time together.
You may also be asked to bring any prior imaging (X‑ray, MRI, CT) or lab results relevant to your joint pain.
The Initial Consultation
Your first visit is typically 60‑90 minutes—much longer than a standard medical appointment. This time allows us to truly understand you, not just your joint pain.
In‑Depth Health History
We’ll sit down together and go far beyond your joints. We’ll ask about:
- When and howyour joint pain started (injury? gradual? after illness?)
- Patterns(morning stiffness? worse with activity? better with rest?)
- Other symptoms(fatigue, brain fog, digestive issues, skin rashes, sleep problems)
- Past medical history(surgeries, infections, autoimmune conditions, trauma)
- Family history(arthritis, autoimmune disease, gut disorders)
- Lifestyle(diet, exercise, stress, sleep, toxin exposure)
- Gut health(bloating, gas, diarrhea, constipation, food sensitivities)
- Prior treatmentsand what has or hasn’t worked
This comprehensive history often reveals clues that point toward root causes like SIBO, leaky gut, hormonal imbalances, or chronic inflammation.
Physical Examination
We’ll perform a focused physical exam of the affected joints, including:
- Range of motion(active and passive)
- Palpationfor tenderness, warmth, or swelling
- Strength testingof surrounding muscles
- Special tests(e.g., for shoulder impingement, meniscal injury, ligament laxity)
- Gait analysisif the knee, hip, or foot is involved
- Postural assessment(often revealing imbalances that contribute to joint stress)
Depending on your symptoms, we may also examine other areas (e.g., spine, opposite joint) to identify compensatory patterns.
Discussion of Goals
What matters most to you? Pain relief? Getting back to golf? Avoiding knee replacement? Sleeping through the night? We’ll clarify your goals and priorities, which will guide our treatment plan.
Diagnostic Testing
Based on your history and exam, we may recommend additional testing to uncover root causes. Unlike conventional orthopedics (which often stops at X‑ray), functional medicine digs deeper.
Common tests we order:
|
Test |
What It Assesses |
|
Advanced imaging (MRI, ultrasound) |
Soft tissue, cartilage, tendons, ligaments |
|
Inflammatory markers (hs‑CRP, ESR, cytokine panel) |
Systemic inflammation |
We tailor testing to your specific presentation.
Creating Your Personalized Plan
By the end of your first visit (or within a few days after test results return), we’ll develop a personalized roadmap that may include:
- Joint‑specific treatments(injections, bracing, physical therapy)
- Regenerative medicine(PRP, hyaluronic acid, peptides)
- IV therapy(anti‑inflammatory, NAD+, sports recovery)
- Lifestyle modifications(stress reduction, sleep optimization, exercise)
- Referrals(to physical therapists, nutritionists, or other specialists as needed)
You’ll leave with a clear understanding of the “why” behind each recommendation and a written plan to follow.
Follow‑Up and Ongoing Care
Functional medicine is not a one‑and‑done visit. Healing takes time, especially when addressing chronic inflammation or gut dysfunction.
- Follow‑up visitsare typically scheduled 4‑8 weeks after the initial consultation to review test results, assess progress, and adjust the plan.
- Ongoing monitoringmay include repeat testing (e.g., inflammatory markers, stool analysis) to track improvement.
- Telemedicine follow‑upsare available for patients who live outside the Charlotte area or prefer virtual visits.
Our goal is to empower you with the tools and knowledge to maintain joint health long after your treatment course ends.
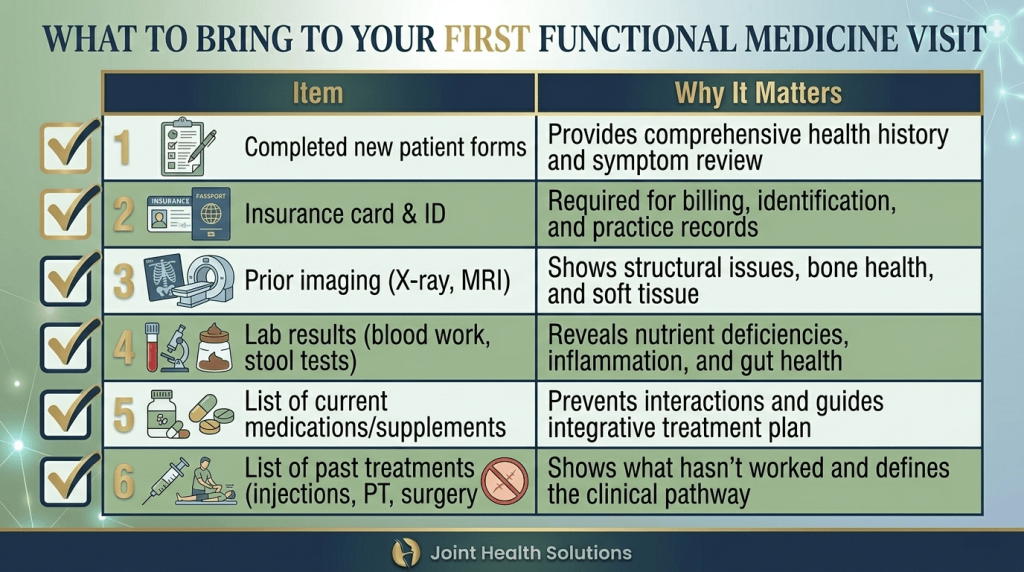
What to Bring
To make the most of your first visit, please bring:
- Completed new patient forms (sent via email)
- Insurance card and photo ID
- Any prior imaging (X‑ray, MRI, CT) on CD or digital access
- Any recent lab results (blood work, stool tests)
- A list of all current medications, supplements, and over‑the‑counter products
- A list of past treatments for your joint pain (injections, physical therapy, surgeries)
- Your questions and goals
Don’t worry if you don’t have everything – we can still do a thorough evaluation and request records later.
Add Your Heading Text Here
How long is the first appointment?
Approximately 60‑90 minutes. This allows time for a comprehensive history, physical exam, and discussion of initial recommendations.
Will I receive treatment on the first visit?
Sometimes. If we perform an injection (e.g., cortisone, hyaluronic acid) or order immediate tests, we can often do that same day. However, many treatments (like PRP, gut protocols, or supplements) require test results first.
Do I need a referral?
No, we accept patients directly. However, if your insurance requires a referral for specialist visits, please obtain one beforehand.
Do you accept insurance?
We accept many insurance plans for medical services (office visits, injections, etc.). Functional medicine testing and IV therapy may not be covered. Our team will verify your benefits before your visit. We also have private pay options for patients opting out of medical insurance.
What if I don’t have prior imaging or lab work?
That’s fine. We can order what’s needed after the visit.
Can I bring someone with me?
Yes. Many patients bring a spouse, adult child, or friend to help take notes and provide support.
Will you prescribe pain medications?
We focus on treating the root cause of pain, not masking it with opioids or long‑term narcotics. In select cases, we may prescribe non‑narcotic pain relievers as a bridge.
How soon will I feel better?
It depends on the underlying cause. Some patients notice improvement within 1‑2 weeks after dietary changes or injections. Others with chronic gut issues or hormone imbalances may take 2‑3 months to see significant change.
What’s the difference between functional medicine and conventional orthopedics?
Conventional orthopedics focuses on the joint structure (X‑ray, MRI, surgery, injections). Functional medicine adds the root‑cause layer: inflammation, gut health, nutrition, hormones, and lifestyle.
How do I schedule?
Call the Joint Health Solutions office at 704-833-3566 or use the online booking link. We’ll send you the new patient packet and confirm your appointment.
Approximately 60‑90 minutes. This allows time for a comprehensive history, physical exam, and discussion of initial recommendations.
Sometimes. If we perform an injection (e.g., cortisone, hyaluronic acid) or order immediate tests, we can often do that same day. However, many treatments (like PRP, gut protocols, or supplements) require test results first.
No, we accept patients directly. However, if your insurance requires a referral for specialist visits, please obtain one beforehand.
We accept many insurance plans for medical services (office visits, injections, etc.). Functional medicine testing and IV therapy may not be covered. Our team will verify your benefits before your visit. We also have private pay options for patients opting out of medical insurance.
That’s fine. We can order what’s needed after the visit.
Yes. Many patients bring a spouse, adult child, or friend to help take notes and provide support.
We focus on treating the root cause of pain, not masking it with opioids or long‑term narcotics. In select cases, we may prescribe non‑narcotic pain relievers as a bridge.
It depends on the underlying cause. Some patients notice improvement within 1‑2 weeks after dietary changes or injections. Others with chronic gut issues or hormone imbalances may take 2‑3 months to see significant change.
Conventional orthopedics focuses on the joint structure (X‑ray, MRI, surgery, injections). Functional medicine adds the root‑cause layer: inflammation, gut health, nutrition, hormones, and lifestyle.
Call the Joint Health Solutions office at 704-833-3566 or use the online booking link. We’ll send you the new patient packet and confirm your appointment.
Sources
-
Institute for Functional Medicine – What to Expect During a Functional Medicine Visit.
🔗 www.ifm.org/functional-medicine/what-to-expect/ -
Cleveland Clinic – Functional Medicine: What It Is and How It Works.
🔗 my.clevelandclinic.org/health/treatments/23032-functional-medicine -
Mayo Clinic – Integrative and functional medicine.
🔗 www.mayoclinic.org/medical-professionals/functional-medicine -
Patient Education (Joint Health Solutions) – New Patient Information.



